"Silent" Autonomic Dysreflexia (AD) & Cerebrovascular Damage
Brief Summary of the Problem
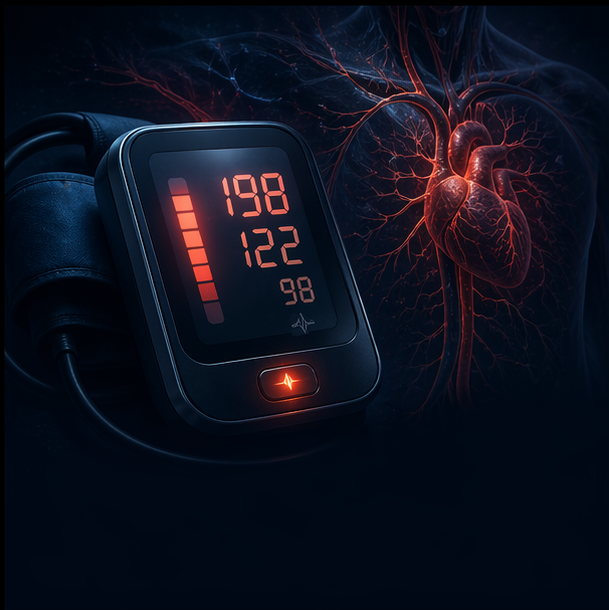
Autonomic Dysreflexia (AD) is a potentially life-threatening medical emergency unique to individuals with spinal cord injuries (SCI) at or above the sixth thoracic vertebra (T6). It is characterized by an exaggerated, uncontrolled spike in blood pressure triggered by a noxious stimulus below the level of injury. While classic AD presents with severe warning signs like a pounding headache, profuse sweating, and upper-body flushing, research reveals that up to 40% to 60% of AD episodes are entirely "silent" (asymptomatic). Because the patient feels completely normal, these extreme blood pressure spikes go undetected and untreated, acting as a repetitive "hammer" against the brain's delicate blood vessels and causing long-term structural cerebrovascular damage, stroke, and cognitive decline.
What is Going Wrong & Why
AD is the result of a massive "communication breakdown" and maladaptive rewiring within the nervous system. When a painful or irritating stimulus occurs below the level of the injury (most commonly an overfull bladder, bowel impaction, or skin issue), sensory nerves send distress signals up the spinal cord. Because the spinal cord is damaged, these signals cannot reach the brain.
Instead, the signals "short-circuit" and trigger a massive reflex in the sympathetic nervous system below the injury. This causes widespread, intense constriction of the blood vessels (vasoconstriction), particularly in the massive network of blood vessels in the abdomen (the splanchnic bed). This rapid constriction forces a massive volume of blood upward, causing systemic blood pressure to skyrocket.
The brain detects this dangerous pressure spike via sensors in the neck (baroreceptors) and attempts to fix it by sending parasympathetic "calming" signals downward. However, these signals are physically blocked by the spinal cord lesion. The brain can only slow the heart rate (bradycardia) and dilate blood vessels above the injury (causing the classic flushed face and headache), while the dangerous vasoconstriction below the injury continues unabated.
Furthermore, the spinal cord actually rewires itself to make this reflex worse over time. Following an SCI, primary pain fibers (C-fibers) and specific interneurons (V2a) undergo aberrant sprouting, creating new, hypersensitive circuits that amplify these sympathetic reflexes. But why are so many episodes silent? Over time, the repeated cardiovascular trauma from AD causes the body's baroreceptors to become desensitized. The brain's alarm system essentially fatigues, allowing blood pressure to shoot up without triggering the usual headache or slowing the heart rate.
The Implications, Long-Term Problems, and Confounding Issues
The consequences of living with unmanaged, silent AD are devastating to brain health. The constant "roller coaster" of blood pressure—dropping too low from orthostatic hypotension and spiking violently from silent AD—causes inward remodeling and stiffening of the Middle Cerebral Artery (MCA). This repetitive shear stress leads to blood-brain barrier (BBB) leakage, cerebral microhemorrhages (tiny brain bleeds), and transient cerebral hypoperfusion (starving the brain of oxygen). Ultimately, this vascular damage drives cognitive decline ("brain fog") and increases the risk of a stroke by an astounding 300% to 400% compared to the general population.
The Confounding Issue for Healthcare Providers (The "Normal" Blood Pressure Trap)
Standard medical guidelines classify a "normal" blood pressure as 120/80 mmHg. However, because individuals with high-level SCI lack descending sympathetic control, their resting baseline blood pressure is frequently much lower, typically ranging from 90/60 to 110/70 mmHg.
An AD episode is clinically defined as a sudden increase in systolic blood pressure of 20 to 40 mmHg above the patient's baseline. Therefore, an SCI patient experiencing a silent AD episode might sit in a doctor's office with a reading of 130/85 mmHg. A primary care provider unfamiliar with SCI physiology will document this as "perfectly normal" or "mild prehypertension," completely failing to recognize that the patient is in the middle of a life-threatening hypertensive crisis capable of causing a stroke.
Current Advice, Treatments & Research Trends
The management of AD is rapidly shifting from purely reactive emergency responses to proactive, technology-driven prevention.
- Current Emergency Management: When AD is suspected, the immediate response must be to sit the patient upright with their legs dangling (to use gravity to pull blood away from the brain), loosen all restrictive clothing, and immediately search for and resolve the trigger (e.g., draining the bladder or clearing the bowel). If blood pressure remains dangerously high, rapid-acting, short-duration antihypertensives like sublingual nifedipine or nitroglycerin paste (which can be quickly wiped off) are administered.
- The Major Flaw with the Current Standard of Care: The major flaw with the current standard of care for Autonomic Dysreflexia (AD)—using rapid-acting drugs like nifedipine—is that they are "blunt instruments" that cause systemic vasodilation. Because these drugs persist in your system after the AD trigger is resolved, they frequently cause severe "rebound hypotension" (a sudden, dangerous crash in blood pressure), which is especially risky since people with high-level SCI already have a low resting blood pressure.
- Prazosin (The Alpha-1 Blocker): A promising drug that may solve this specific problem is Prazosin. Currently in Phase 2 trials for AD prophylaxis (preventative use for predictable triggers like bowel programs or sperm retrieval), Prazosin is a selective alpha-1 blocker. Research shows that Prazosin effectively blunts the sympathetic blood pressure surge (the high) without obliterating your resting blood pressure, allowing patients to successfully avoid the dangerous post-AD hypotensive "crash" commonly seen when nifedipine is taken proactively.
- Mirabegron (The Beta-3 Agonist): Instead of trying to lower systemic blood pressure during an attack, researchers are repurposing advanced urological drugs to proactively eliminate the trigger of the attack. Mirabegron is emerging as a superior alternative to older anticholinergics (like oxybutynin). It works by targeting beta-3 adrenergic receptors to relax the bladder's detrusor muscle during the storage phase. Because high bladder pressure is the primary trigger for AD, Mirabegron acts as a specific prophylactic; trials show it significantly reduces AD frequency and severity without causing the rebound hypotension associated with systemic blood pressure drugs.
- "Dual-Purpose" Botox & Bladder Gene Therapy (EG-427): Targeted interventions directly into the bladder are being validated as powerful cardiovascular protectants.
- Intradetrusor OnabotulinumtoxinA (Botox): Clinical trials have recently quantified that Botox does more than just stop incontinence; by chemically denervating the afferent arm of the reflex loop, it effectively "silences" the bladder as an AD trigger for 6 to 9 months, drastically blunting hypertensive surges during episodes.
- EG-427 (Gene Therapy): Taking this a step further, an upcoming therapy currently in Phase 1b/2a trials uses a modified virus vector to deliver the botulinum toxin gene directly into sensory neurons. This acts as a biologic drug intended to provide long-lasting, permanent inhibition of the overactive bladder reflexes that cause AD.
- The "Bionic Baroreflex" (Targeted Epidural Stimulation): The most exciting breakthrough in AD research is the development of implantable Epidural Electrical Stimulation (EES) devices (such as the ARC-IM). Researchers have mapped the exact "hemodynamic hotspot" in the lower thoracic spinal cord (T11-L1) responsible for blood pressure regulation. By providing continuous, closed-loop electrical stimulation to this specific region, these implants act as an artificial baroreflex, successfully competing with the maladaptive AD circuits to instantly stabilize blood pressure and prevent dangerous spikes.
- AI Wearables & Early Detection: Because silent AD provides no warning, researchers are developing AI-driven wearables to detect episodes before blood pressure peaks. For example, systems analyzing Skin Nerve Activity (SKNA) and heart rate variability can accurately predict the onset of an AD event by detecting the invisible sympathetic surge, serving as an "early warning alarm" for patients. Wireless, catheter-free bladder sensors (like the UroMonitor) are also being tested to alert patients of dangerous bladder pressures before they trigger an AD spike.
- Pharmacological Repurposing: Rather than giving systemic blood pressure drugs that cause fatigue, research is proving that proactively treating the triggers stops the disease. The recent use of bladder-relaxing drugs like Fesoterodine (an antimuscarinic) or targeted intradetrusor Botox injections has been clinically proven to reduce the frequency of AD episodes by up to 75% simply by preventing the bladder spasms that initiate the reflex. Furthermore, cutting-edge therapies are exploring the use of sTNFα inhibitors (like XPro1595) shortly after injury to block the neuroinflammation that causes the AD circuits to miswire in the first place.
Neurogenic Osteoporosis & The "Calcium/Stone Paradox"
Brief Summary of the Problem
Following a spinal cord injury (SCI), the sudden loss of mechanical weight-bearing causes the skeleton below the level of injury to rapidly deteriorate—a condition known as neurogenic osteoporosis. Within the first year, individuals can lose a massive percentage of their bone mineral density, particularly around the knees. As these bones break down, they release massive amounts of calcium into the bloodstream, which is then filtered by the kidneys and dumped into the urine (a state called hypercalciuria). This creates a highly dangerous double-edged sword: the paralyzed limbs become incredibly fragile and prone to fractures from minor movements, while the flooded kidneys become a prime breeding ground for severe kidney stones.
What is Going Wrong & Why
Your bones are living tissue constantly being remodeled by a delicate balance of "builder" cells (osteoblasts) and "demolition" cells (osteoclasts). In a healthy body, the physical strain of gravity and walking tells the builders to keep working.
When you sit in a wheelchair, that mechanical strain disappears. Deep inside your bones, sensor cells realize they are no longer bearing weight and release highly destructive proteins called Sclerostin and DKK-1. These proteins act as a massive "stop sign" that entirely shuts down the bone-building osteoblasts. At the same time, the signals controlling the demolition crew (osteoclasts) go into overdrive. Because the demolition vastly outpaces the building, the bone structure is rapidly eaten away, and all the stored calcium is flushed into the bloodstream and out through the urinary tract.
The Implications, Long-Term Problems, and Confounding Issues
This rapid bone breakdown leads to a high risk of lower extremity fragility fractures, which can occur from something as simple as a spasm or a wheelchair transfer. Meanwhile, the saturated levels of calcium sitting in the bladder lead to recurrent, often painless, kidney and bladder stones.
Confounding Issue 1: The "Calcium/Stone Paradox" (Why fasting from calcium is counter-productive)
The most dangerous confounding issue is how patients and even some doctors approach the kidney stone problem. Standard logic dictates: "If I have too much calcium in my urine making kidney stones, I should consume less dietary calcium to lower it."
This is entirely wrong and highly counter-productive. Starving yourself of dietary calcium actually accelerates kidney stone formation and destroys your remaining bone density.
Here is why: Many healthy plant foods contain a chemical called oxalate. When you consume a normal amount of dietary calcium (like drinking a glass of milk), that calcium binds to the oxalates right there in your stomach and intestines. Because they are locked together, your body safely excretes them in your stool.
If you stop eating dietary calcium, those oxalates have nothing to bind to in your gut. They get absorbed directly into your bloodstream, travel to your kidneys, and bind to the calcium that is already leaking from your paralyzed bones. The result? You form highly dangerous calcium-oxalate kidney stones. Furthermore, if you restrict dietary calcium, your body is forced to steal even more calcium from your already-weakened skeleton to survive, rapidly worsening your osteoporosis.
Confounding Issue 2: The DXA Scan Glitch
Standard medical practice for diagnosing osteoporosis involves a DXA scan of the lumbar spine and the hip. However, for someone with an SCI, scanning the spine is dangerously misleading. In SCI, the lumbar spine often looks falsely healthy, or even artificially dense, due to wheelchair loading, spinal hardware, or osteoarthritis. The actual severe bone loss occurs around the knees (the distal femur and proximal tibia). If a healthcare provider relies on a standard spine scan, they will likely miss severe neurogenic osteoporosis entirely.
Current Advice, Treatments & Research Trends
To successfully protect the bones and prevent stones, clinical management completely flips standard able-bodied advice on its head.
- Dietary Shifts (Eat Calcium, Cut Salt): Clinical guidelines strongly advise against restricting calcium. SCI patients should maintain a normal, healthy calcium intake (around 1,000 to 1,200 mg daily), preferably from dairy or food rather than supplement pills, to bind oxalates in the gut. To actually stop the kidneys from dumping calcium, patients must strictly limit sodium (salt) to less than 1.5 grams daily, as salt actively forces the kidneys to excrete calcium. Furthermore, massive hydration is required to produce at least 2 to 2.5 liters of urine daily to keep any minerals diluted.
- Diagnostic Shifts for Providers: The 2019 International Society for Clinical Densitometry (ISCD) explicitly mandates that individuals with SCI must have DXA scans that specifically measure the distal femur and proximal tibia (just above and below the knee) to accurately predict fracture risk.
- Bionic and Passive Loading: Because simple passive standing frames have largely failed to rebuild bone, researchers are proving that the bones need dynamic, pulling forces to grow. Therapies like Functional Electrical Stimulation (FES) cycling, or specialized machine-driven passive-isokinetic cycling, are being used to physically force paralyzed muscles to contract against resistance, artificially signaling the bones to rebuild.
- Targeted Pharmacology: Current osteoporosis drugs (like bisphosphonates) have had mixed success in SCI because they freeze bone remodeling entirely. The newest research frontier involves targeted antibodies that fix the broken cellular signals. Drugs like Denosumab (which blocks osteoclast formation) have shown success in increasing sublesional bone mass. More excitingly, emerging therapies like Anti-Sclerostin antibodies (which remove the "stop sign" on bone building) and Anti-Siglec-15 (NP159) are proving in trials that they can completely halt bone loss by shutting down the demolition crew while simultaneously promoting the bone builders.
8. Chronic Neuropathic Pain & Systemic Sensitization
Brief Summary of the Problem
Chronic pain affects an estimated 60% to 80% of the population with a traumatic spinal cord injury (SCI). While some of this is standard musculoskeletal ache, the most debilitating and prevalent form is neuropathic pain—a relentless, burning, or stabbing sensation caused directly by the lesion to the somatosensory nervous system. Unlike acute pain that protects the body from harm, chronic neuropathic pain in SCI is a "maladaptive" disease state where the nervous system becomes systemically sensitized. It fires continuous, false alarm signals that are highly resistant to traditional painkillers, creating a devastating cycle that severely impairs sleep, limits rehabilitation, and drives clinical depression.
What is Going Wrong & Why
The onset of chronic neuropathic pain is not just a severed wire; it is an active, toxic rewiring of the spinal cord and brain driven by several compounding mechanisms:
- The "Flipped" Switch (Loss of Chloride Homeostasis): In a healthy spinal cord, a neurotransmitter called GABA acts as the "brakes" (an inhibitory signal) to stop pain signals from overwhelming the brain. This relies on a microscopic pump called KCC2, which constantly clears chloride out of the nerve cells. After an SCI, KCC2 is drastically downregulated, while another pump (NKCC1) goes into overdrive, trapping chloride inside the cell. Because of this imbalance, when GABA attaches to the cell, it acts as an "accelerator" instead of a brake. The nervous system becomes hyperexcitable, amplifying normal touch or internal signals into severe pain.
- Aberrant Sprouting and Neurotrophin Overload: Following the injury, high levels of Nerve Growth Factor (NGF) and Brain-Derived Neurotrophic Factor (BDNF) are released in the spinal cord. This causes primary pain fibers (C-fibers) to abnormally sprout and form new, inappropriate connections in the dorsal horn (the sensory relay station of the spinal cord), permanently "hard-wiring" a hypersensitive pain circuit. Additionally, the accumulation of Tau proteins within spinal neurons actively upregulates inflammatory pain pathways.
- The Adipokine & Gut Amplifiers: The pain is continuously fed by systemic inflammation. Metabolically toxic visceral fat (neurogenic obesity) secretes pro-inflammatory cytokines (like TNF-α and IL-6) that directly sensitize the voltage-gated sodium channels (NaV) on nociceptive (pain) nerves. Simultaneously, SCI-induced gut dysbiosis reduces the body's natural production of soothing neurotransmitters like serotonin and GABA, while leaking inflammatory endotoxins into the blood that further lower the pain threshold.
The Implications, Long-Term Problems, and Confounding Issues
Living with systemic sensitization places the central nervous system in a state of constant exhaustion, leading to severe cognitive "brain fog," profound sleep disturbances, and an elevated risk of mood disorders.
Confounding Issue 1: The Obesity/Pain Feedback Loop
In the general population, a doctor might view weight and pain as somewhat independent. In SCI, neurogenic obesity and neuropathic pain share a reciprocal, vicious biological loop. The extreme loss of muscle and increase in visceral fat directly pumps out the inflammatory adipokines that physically alter nerve receptors to feel more pain. That severe pain then prevents the patient from engaging in physical activity, which increases the toxic visceral fat, which then pumps out even more pain-sensitizing chemicals.
Confounding Issue 2: The Medication Trap
Standard medical advice for neuropathic pain heavily relies on Gabapentinoids (like gabapentin or pregabalin) or long-term opioids. In the SCI population, this is a dangerous trap.
Because of the "Kidney Test Trap," doctors often overprescribe gabapentin, leading to severe sedation, daytime sleepiness, and loss of motor coordination (which increases wheelchair falls). Furthermore, long-term opioids do not effectively target the root nerve damage; instead, they paralyze the gut (worsening inflammatory dysbiosis), completely suppress the body's testosterone production (accelerating muscle loss), and can actually induce hyperalgesia (making the nervous system even more sensitive to pain over time).
Current Advice, Treatments & Research Trends
The management of SCI neuropathic pain is moving away from sedating the brain and instead focusing on actively reprogramming the broken spinal circuits and cooling systemic inflammation.
- Pharmacological Reprogramming (KCC2 Potentiators): Rather than using blunt-force drugs that cause "brain fog," the newest frontier in SCI pain research involves targeted drugs that fix the broken chloride pumps. Molecules like CLP290 and emerging oral therapies (such as those being developed by Axonis Therapeutics) are designed to reactivate the KCC2 pump. By pumping the chloride back out of the cells, these drugs restore the natural inhibitory "brakes" of the spinal cord, showing immense promise in preclinical trials for relieving both spasticity and neuropathic pain without sedating the patient.
- Neuromodulation (Bypassing the Pain): Both implanted Epidural Electrical Stimulation (EES) and non-invasive Transcutaneous Spinal Cord Stimulation (tcSCS) are proving highly effective at overriding these abnormal pain circuits. The electrical pulses actively recruit local GABAergic mechanisms to suppress the overactive pain neurons. Additionally, repetitive Transcranial Magnetic Stimulation (rTMS) applied directly to the motor cortex of the brain (M1) is being used to non-invasively rewire how the brain perceives the pain, showing long-lasting reductions in central pain severity and depression scores.
- Targeted Anti-Inflammatory Diets & Microbiome Therapy: Because systemic inflammation physically drives nerve sensitization, clinical trials are shifting toward diet as medicine. Implementing a strict 12-week anti-inflammatory diet has been clinically shown to significantly reduce systemic inflammatory biomarkers and actively lower neuropathic pain severity in chronic SCI patients. Furthermore, researchers are exploring targeted probiotics to restore the gut's ability to synthesize natural serotonin and GABA to elevate the patient's biological pain threshold.
Neurogenic Obesity, The "BMI Illusion", and the Accelerated Risk of Type 2 Diabetes
Brief Summary of the Problem
Following a spinal cord injury (SCI), the body undergoes a radical and permanent shift in its composition. Even if a person’s total body weight remains stable, profound muscle loss below the level of injury is rapidly replaced by metabolically toxic visceral fat. This creates a dangerous state of "neurogenic obesity" that is often entirely masked by a seemingly healthy Body Mass Index (BMI). This hidden fat acts as an inflammatory factory that, when combined with the massive loss of muscle tissue, destroys the body's ability to process blood sugar. Consequently, individuals with SCI face a much younger onset and a significantly higher prevalence of Type 2 Diabetes and cardiometabolic disease compared to the general population.
What is Going Wrong & Why
The rapid onset of neurogenic obesity and subsequent diabetes is driven by a two-front assault on the body's metabolism:
- The Loss of the "Glucose Sink": In a healthy body, skeletal muscle is the primary "sink" or reservoir for absorbing circulating blood sugar, responsible for taking up to 70% of the body's glucose. When motor signals are severed by an SCI, the paralyzed muscle undergoes an obligatory and severe atrophy, with individuals losing nearly 50% of the cross-sectional area of their muscle below the injury within just six weeks. Because the body's primary storage tank for glucose is suddenly gone, sugar remains trapped in the bloodstream.
- The Rise of Toxic Fat (Adipokines & NEFAs): The drastically lowered resting metabolic rate from this muscle loss causes rapid fat accumulation, even if daily caloric intake remains the same. This new fat primarily packs around the internal organs (visceral fat) and infiltrates the remaining atrophied muscle (intramuscular fat). These specific fat deposits are not just passive storage; they are active endocrine organs that pump out inflammatory signals (adipokines like IL-6 and TNF-α) and non-esterified fatty acids (NEFAs). These toxic chemicals physically block the intracellular transport of plasma glucose in the remaining healthy tissues, creating severe, system-wide insulin resistance.
The Implications, Long-Term Problems, and Confounding Issues
Because of these compounding factors, obesity and insulin resistance are strikingly comorbid in the SCI population. The resulting Type 2 Diabetes drives severe, long-term consequences, accelerating atherogenesis (plaque buildup in arteries), cardiovascular disease, and compounding poor wound healing (such as pressure injuries) due to impaired microcirculation.
Confounding Issue 1: The BMI Illusion
In the general population, obesity is diagnosed using a BMI threshold of ≥ 30 kg/m². However, the standard BMI scale is fundamentally flawed and dangerous for the SCI population because it assumes a normal ratio of muscle to fat. Because heavy muscle has been replaced by lighter fat, an individual with a chronic SCI can look thin on the outside and have a "perfectly healthy" BMI of 23, but actually possess a body fat percentage that makes them clinically obese.
Confounding Issue 2: The DXA Scan Glitch (Explained Simply)
You might think an advanced medical scan would catch this hidden fat, but even standard technology can fail SCI patients. The medical literature notes that standard Dual-Energy X-ray Absorptiometry (DXA) body scans can mislead doctors by incorrectly grouping intermuscular adipose tissue (IMAT) in with healthy truncal muscle, falsely overestimating the patient's lean mass.
Here is the layman's translation of what that means:
Think of a high-quality cut of steak that has a lot of "marbling"—thin white streaks of fat woven directly inside the red meat. After an SCI, your paralyzed muscles develop this exact kind of fat marbling (this is the IMAT). When a standard DXA scanner looks at your body, it is simply not smart enough to separate those tiny streaks of fat from the actual muscle fibers. It accidentally counts that hidden fat as healthy muscle. Because of this machine "glitch," a doctor might look at your scan results and say, "Great news, you have plenty of healthy muscle mass!" when in reality, a large portion of that "muscle" is actually toxic, marbled fat that is actively causing insulin resistance and pushing you toward diabetes.
Current Advice, Treatments & Research Trends
To mitigate the long-term effects of neurogenic obesity and diabetes, clinical focus is shifting toward specialized diagnostics, targeted nutrition, and bionic rehabilitation.
- Diagnostic Shifts for Providers: Healthcare providers must abandon standard obesity charts. For individuals with SCI, a BMI of ≥ 22 kg/m² must be recognized as the clinical threshold for obesity and high cardiometabolic risk. Furthermore, because SCI patients have unique metabolic profiles, standard fasting glucose tests might miss early diabetes; researchers recommend using a combination of Fasting Glucose, a 2-hour Post-Load Glucose test, and Hemoglobin A1c (HbA1c) to accurately catch insulin resistance before it becomes full-blown diabetes.
- Targeted Nutritional Therapy: Extreme fasting is highly discouraged as it causes further dangerous losses of bone and lean muscle mass. Instead, research supports a "metabolic-first" dietary approach featuring a higher protein-to-calorie ratio to preserve remaining lean mass, and a strict reduction of high-sugar/high-glycemic foods to combat insulin resistance and neutralize the inflammatory adipokines being released by visceral fat.
- Rebuilding the Metabolic Sink: To combat the drastically lowered metabolic rate and rebuild the body's "glucose sink," clinicians are utilizing Functional Electrical Stimulation (FES) therapies (like FES cycling or rowing). FES forces paralyzed muscles to contract against resistance. This artificial exercise recruits "GLUT4 receptors" to the surface of the muscle cells, which actively pulls excess glucose out of the blood, acting as a massive metabolic sink that directly fights diabetes and significantly reduces systemic inflammation.
7. Orthostatic and Postprandial Hypotension (Blood Pooling)
Brief Summary of the Problem
Following a high-level spinal cord injury (SCI), the cardiovascular system frequently loses its ability to fight gravity and digest food without severely compromising blood flow to the brain. This manifests as two distinct but related conditions: Orthostatic Hypotension (OH), a sudden, dangerous crash in blood pressure when sitting or standing up, and Postprandial Hypotension (PPH), a severe blood pressure drop occurring within two hours of eating a meal. While able-bodied individuals rarely experience these extreme drops, individuals with SCI suffer from massive internal "blood pooling." Over time, this chronic starvation of oxygen to the brain drives debilitating daytime fatigue, "brain fog," and significantly increases the risk of early-onset cognitive decline and vascular dementia.
What is Going Wrong & Why
The root cause of both OH and PPH is the severance of the brain's connection to the sympathetic nervous system.
In a healthy body, whenever you sit up or stand, gravity tries to pull your blood down into your legs. Your brain instantly detects this and sends sympathetic signals down the spinal cord to constrict (squeeze) the blood vessels in your legs and abdomen, pushing the blood back up to your heart and head. After an SCI, these descending signals are physically blocked.
Without this sympathetic "squeeze," massive amounts of blood helplessly pool in the lower extremities and the splanchnic bed (the massive network of blood vessels in your abdomen). Because the blood is trapped below the injury, the volume of blood returning to the heart plummets, causing cardiac output and arterial blood pressure to crash.
Postprandial Hypotension (The Digestion Crash): PPH operates on a similar mechanism. When you eat, the body naturally diverts a large volume of blood to the gut to aid in digestion. In an able-bodied person, the heart beats slightly faster and peripheral blood vessels constrict to compensate for this diverted blood. In an SCI patient, the blood rushes to the gut but the paralyzed body cannot constrict other vessels to compensate, resulting in a severe, sustained drop in blood pressure (often ≥ 20 mmHg) that can last up to two hours after a meal.
The Implications, Long-Term Problems, and Confounding Issues
The immediate implications of this blood pooling are dizziness, blurred vision, and fainting during wheelchair transfers or after eating. However, the long-term consequences are far more insidious. Chronic systemic hypotension and repetitive drops in blood pressure lead to "transient cerebral hypoperfusion"—meaning the brain is chronically starved of adequate blood flow and oxygen. Over decades, this vascular damage directly drives cognitive deficits in memory, attention, and processing speed, and accelerates the risk of vascular dementia.
Confounding Issue 1: Asymptomatic "Silent" Crashes
A major confounding issue for healthcare providers is that up to 96% of PPH episodes and a massive percentage of OH episodes in the SCI population are entirely asymptomatic. A patient's blood pressure can crash to dangerously low levels (e.g., a systolic blood pressure below 90 mmHg), starving their brain of oxygen, without the patient feeling dizzy or lightheaded. Providers must realize that the absence of dizziness does not mean the brain is adequately perfused.
Confounding Issue 2: The Salt Paradox
Standard medical advice for the general population is to heavily restrict dietary salt to prevent high blood pressure. For a high-level SCI patient suffering from OH, this advice is backwards. Because they lack vascular tone, SCI patients often require increased salt and fluid intake (particularly in the mid-morning) to artificially expand their blood volume and prevent hypotensive crashes.
Confounding Issue 3: The Medication Trap
Treating OH with standard blood-pressure-raising drugs (like Midodrine) presents a dangerous tightrope walk. Because the SCI cardiovascular system is so unstable, a drug taken to prevent an OH crash during the day can cause severe, life-threatening supine hypertension when the patient lies down to sleep, or dangerously interact with Autonomic Dysreflexia (AD) triggers.
Current Advice, Treatments & Research Trends
The management of blood pooling is advancing rapidly, moving from basic compression garments to highly advanced bionic implants.
- Mechanical and Dietary Baselines: The current standard of care involves using medical-grade abdominal binders and compression stockings to physically compress the capacitance beds in the abdomen and legs, fighting gravity manually. Clinically, adjusting meal sizes (eating smaller, more frequent meals) and utilizing targeted salt and water loading are first-line defenses against PPH and OH.
- Bionic Muscle Pumps (FES): Because paralyzed legs can no longer physically pump blood back to the heart, therapies utilizing Functional Electrical Stimulation (FES) are being deployed. By applying electrical currents to the leg muscles during orthostatic challenges or cycling, FES forces the muscles to contract, artificially restoring the "skeletal muscle pump" to facilitate venous blood return and stabilize blood pressure.
- The "Neuroprosthetic Baroreflex" (Targeted Epidural Stimulation): The most groundbreaking trend in SCI cardiovascular research is the use of implantable Epidural Spinal Cord Stimulation (EES) devices (like the ONWARD ARC-IM). Researchers discovered that by targeting a specific "hemodynamic hotspot" in the lower thoracic spinal cord (T11-L1), a closed-loop implant can automatically detect a drop in blood pressure and instantly deliver electrical pulses to constrict the splanchnic blood vessels. In recent 2025 clinical trials, this implant successfully eradicated debilitating hypotensive crashes, allowing patients to sit up and eat without "brain fog" or fainting.
- Emerging Non-Invasive Therapies: Non-invasive clinical trials are also showing that mild, acute intermittent hypoxia (tAIH)—having the patient breathe brief periods of lower-oxygen air—can strengthen autonomic control and drastically improve orthostatic tolerance. Additionally, Low-Intensity Focused Ultrasound (LIFU) is being actively researched as a futuristic, non-invasive way to sonicate the spinal cord to quickly raise or lower blood pressure on demand.
The Gut-Spinal Cord Axis, Dysbiosis, & "Leaky Gut"
Brief Summary of the Problem
Following a spinal cord injury (SCI), the communication network between the central nervous system and the gastrointestinal tract is severely disrupted—a bidirectional relationship known as the "Gut-Spinal Cord Axis". This loss of autonomic control slows digestion to a crawl, creating a stagnant environment that fosters the overgrowth of harmful bacteria while depleting beneficial ones. This imbalance, called gut dysbiosis, physically breaks down the intestinal wall, creating a "leaky gut" that allows toxic bacterial byproducts to flood into the bloodstream. These toxins travel back to the spinal cord and brain, acting as a massive systemic amplifier for neuroinflammation that halts neurological repair and drives devastating secondary complications like depression and neuropathic pain.
What is Going Wrong & Why
The onset of "leaky gut" and dysbiosis is driven by mechanical, chemical, and medical factors:
- Loss of the Enteric "Conveyor Belt": SCI disrupts the supraspinal and autonomic nerve signals that control the gut, dramatically increasing colonic transit time (e.g., from a standard 24–48 hours up to 80–120 hours). This prolonged stagnation alters the gut's pH and microenvironment, making it hostile to healthy microbes and highly favorable to opportunistic pathogens.
- Microbial Dysbiosis & SCFA Depletion: The gut normally relies on beneficial bacteria (like Lactobacillus and Bifidobacterium) to ferment dietary fiber into Short-Chain Fatty Acids (SCFAs) such as butyrate, acetate, and propionate. SCFAs are crucial because they nourish the intestinal lining and actively suppress inflammation. After SCI, these beneficial bacteria plummet, while pro-inflammatory, opportunistic bacteria (like Escherichia coli and Clostridium) proliferate. The resulting severe drop in SCFAs leaves the gut wall vulnerable and malnourished.
- The Antibiotic Wipeout: SCI patients frequently require broad-spectrum antibiotics to fight off recurrent UTIs, pneumonia, or wound infections. While necessary, these drugs indiscriminately destroy the remaining beneficial gut flora, exacerbating the dysbiosis and allowing resistant pathogens to thrive in the vacuum.
The Implications, Long-Term Problems, and Confounding Issues### The "Leaky Gut" and Metabolic Endotoxemia
Because of the lack of SCFAs and the overgrowth of harmful bacteria, the tight junction proteins (like occludin and claudins) that normally seal the intestinal wall begin to break down. This allows Lipopolysaccharides (LPS)—highly toxic structural components from the cell walls of harmful Gram-negative bacteria—to literally leak through the intestinal wall and into the systemic bloodstream.
Systemic Inflammation & Blocked Neural Repair
Once in the blood, LPS acts as a systemic poison. It binds to Toll-Like Receptors (specifically TLR4) on the body's immune cells, triggering the NF-κB signaling pathway and activating the NLRP3 inflammasome. This causes a massive release of pro-inflammatory cytokines (like IL-1β, IL-6, and TNF-α). Because SCI also increases the permeability of the blood-spinal cord barrier, these inflammatory signals and endotoxins easily reach the spinal lesion. There, they activate spinal microglia into a chronic destructive state, accelerating neuronal cell death, suppressing axonal regeneration, and worsening neurological deficits.
Confounding Issue 1: "Silent" Malabsorption
Because the gut moves so slowly and is chronically inflamed, the intestinal villi (the tiny fingers that absorb nutrients) begin to atrophy. Patients can suffer from severe, "silent" malabsorption of critical nutrients like Zinc, Selenium, and Vitamin B12, even if their diet appears perfectly healthy.
Confounding Issue 2: The Fiber Paradox
Standard medical advice for the able-bodied population facing constipation is to simply "eat more fiber". However, in chronic SCI, because the bowel’s motility is paralyzed, adding massive amounts of bulk fiber without precisely and massively increasing water intake creates a dense, immovable roadblock in the gut. This can cause a "megacolon" and severe metabolic bloating as the trapped bacteria ferment the stagnant fiber.
Confounding Issue 3: Neuropathic Pain & Depression
The gut normally produces precursors for critical neurotransmitters like serotonin (5-HT) and GABA. Dysbiosis alters tryptophan metabolism, starving the brain of serotonin, which directly amplifies the severity of neuropathic pain and significantly increases the risk of clinical depression and anxiety in SCI patients.
Current Advice, Treatments & Research Trends
Clinical focus is shifting away from simply treating "constipation" with laxatives, moving toward actively healing the Gut-Spinal Cord Axis to reduce whole-body inflammation.
- Diagnostic Shifts for Providers: Physicians are urged to test for "silent" malabsorption (checking Vitamin B12, Zinc, and Selenium panels). Furthermore, if a patient presents with unexplained systemic inflammation, worsening spasticity, or "brain fog," doctors can test for Small Intestinal Bacterial Overgrowth (SIBO) via breath test, or use a Serum Zonulin test to accurately diagnose Leaky Gut Syndrome.
- Targeted Probiotics and Prebiotics (Synbiotics): Introducing specific probiotic strains (like Lactobacillus rhamnosus and Bifidobacterium longum) combined with prebiotics (like inulin or oat bran) can physically rebuild the gut flora, increase SCFA production, restore the intestinal barrier, and significantly lower circulating inflammatory cytokines.
- Fecal Microbiota Transplantation (FMT): One of the most groundbreaking therapeutic frontiers is FMT—transferring fecal bacteria from a healthy donor into the patient's GI tract to recolonize it. In SCI animal models, FMT successfully reconstructed dysbiotic microbial communities, restored SCFA levels, suppressed the TLR4/NF-κB inflammatory pathways, and even promoted neuronal survival and axonal regeneration, leading to visibly improved locomotor recovery.
- Mechanical Motility (Rehabilitation + Flora): Therapies utilizing targeted aerobic exercise or bionic interventions like Functional Electrical Stimulation (FES) are being paired with microbiota regulation. The physical movement from bionic cycling actively increases intestinal blood flow and physically accelerates gut transit times, providing a mechanical solution to prevent bacterial stagnation and support beneficial flora.
Neurogenic Hypogonadism & Accelerated Biological Aging
Brief Summary of the Problem
Following a spinal cord injury (SCI), the body frequently experiences a profound and permanent endocrine "crash." The central nervous system loses its ability to properly communicate with the glands that produce vital anabolic hormones, particularly testosterone and Growth Hormone. This leads to a state of "neurogenic hypogonadism"—a severe hormonal deficiency occurring decades earlier than natural age-related decline. This hormonal starvation, combined with the extreme physical stress of paralysis, prevents the body from repairing its tissues and forces patients into a state of "accelerated biological aging," where a 35-year-old with an SCI can exhibit the cellular and vascular degradation of a 60-year-old.
What is Going Wrong & Why
The rapid drop in testosterone and the onset of accelerated aging in SCI are driven by a multi-front assault on the Hypothalamic-Pituitary-Gonadal (HPG) axis (the brain's hormone control center):
- The Neurological Disconnect: In healthy individuals, the sympathetic nervous system provides signals to the testes to stimulate Leydig cells (which make testosterone). After an SCI, this descending neural connection is severed, directly impairing testicular function.
- The "Fat Factory" (Aromatization): As discussed with neurogenic obesity, heavy muscle is replaced by visceral fat. Visceral fat contains an enzyme called aromatase. This enzyme actively steals what little testosterone the body is producing and chemically converts it into estradiol (estrogen).
- Systemic Inflammation (The Cytokine Attack): The chronic, low-grade inflammation driven by visceral fat produces cytokines like IL-6 and TNF-α. These inflammatory chemicals travel to the brain and physically suppress the hypothalamus, reducing the release of Luteinizing Hormone (LH), the signal that tells the body to make testosterone.
- The Opioid Shut-Down: Chronic pain is common in SCI, and long-term opioid use (e.g., morphine, oxycodone) has a devastating endocrine side effect. Opioids bind directly to receptors in the brain to inhibit the release of Gonadotropin-Releasing Hormone (GnRH), effectively turning the body's testosterone "thermostat" down to zero.
The Layman's Translation: Your body has a "thermostat" that tells it when to make heat (testosterone and growth hormones) to repair your tissues. The spinal cord injury cuts the wires to the heater. The new visceral fat in your belly acts like bad insulation that actively steals the heat and turns it into cold air (estrogen). Finally, the pain medicine you take is like a guest who keeps manually turning the thermostat off. Because your body can't generate "heat," your cells can't repair themselves, and your body begins to age and break down at a highly accelerated rate.
The Implications, Long-Term Problems, and Confounding Issues
Nearly 46% of men with SCI exhibit low serum total testosterone. Without testosterone and Insulin-like Growth Factor 1 (IGF-1, a marker of Growth Hormone), the body cannot maintain muscle or bone, accelerating severe sarcopenia and neurogenic osteoporosis. This anabolic deficiency also causes profound physical fatigue, cognitive "brain fog," and a vicious cycle where lower testosterone causes more fat gain, which in turn destroys more testosterone.
Confounding Issue 1: The "Hidden" Symptoms
In the able-bodied population, the primary red flags a doctor looks for to diagnose low testosterone are erectile dysfunction (ED) and low libido. However, because individuals with SCI already frequently manage sexual dysfunction and ED due to their nerve damage, this classic warning sign is completely masked. Instead, the symptoms present atypically as an inability to maintain upper-body strength, severe lethargy, and mood changes that are frequently misdiagnosed as clinical depression.
Confounding Issue 2: The Blood Test Trap (Total vs. Free Testosterone)
When an SCI patient complains of fatigue, a doctor might run a standard "Total Testosterone" blood test. Often, this number will come back looking perfectly normal (e.g., 350 ng/dL). However, SCI patients frequently have elevated levels of a protein called Sex Hormone Binding Globulin (SHBG). SHBG acts like a sponge, binding up the testosterone in the blood so the body cannot actually use it. Because of high SHBG and fat-related estrogen conversion, a patient's "Total" testosterone might look fine, but their "Free" (usable) testosterone is actually at starvation levels.
Current Advice, Treatments & Research Trends
- Diagnostic Shifts for Providers: Healthcare providers must not rely solely on Total Testosterone. Patients must advocate for a comprehensive endocrine panel that includes Free Testosterone, Luteinizing Hormone (LH), and SHBG. Furthermore, to assess biological aging and Growth Hormone status, doctors should test for IGF-1 (Insulin-like Growth Factor-1), which is a much better marker of tissue health in SCI than chronological age.
- Testosterone Replacement Therapy (TRT): If symptomatic hypogonadism is confirmed, TRT is highly effective at restoring lean mass, improving insulin sensitivity, and boosting mood. However, it must be carefully monitored. TRT can increase red blood cell production, leading to polycythemia (thick blood), which is particularly dangerous for SCI patients who already have a high risk for blood clots (DVT) and strokes due to poor circulation.
- Opioid-Sparing Strategies: Clinical guidelines strongly suggest tapering off long-term opioids to reverse "opioid-induced androgen deficiency" and allow the brain's GnRH signals to "wake up" and naturally stimulate testosterone production.
- Sleep & Nutritional Interventions: Maximizing sleep quality is heavily emphasized, as this is when the body naturally releases Growth Hormone. Melatonin is frequently recommended not just for sleep, but because it acts as a powerful antioxidant to combat the cellular aging caused by inflammation. Additionally, optimizing Zinc, Magnesium, and Vitamin D intake has been shown in research to actively support the remaining natural hormone production pathways and modulate the "nutrition-microbiota-androgen" axis.
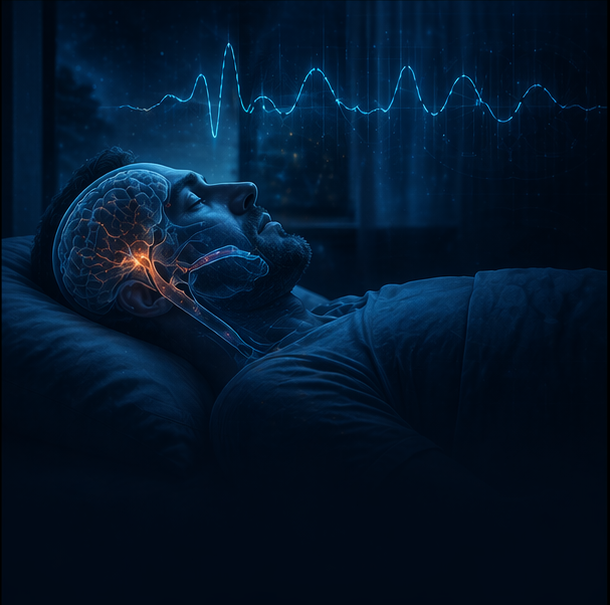
9. Respiratory Dysfunction & Central Sleep Apnea
Brief Summary of the Problem
Respiratory complications are the absolute leading cause of morbidity and mortality for individuals living with spinal cord injuries (SCI), particularly in the first year after injury and continuously throughout life. The severance of motor signals to the torso paralyzes the primary and accessory breathing muscles, leading to severe restrictive lung disease and the complete inability to produce an effective cough. Furthermore, during sleep, profound neurological instability leads to staggeringly high rates of sleep-disordered breathing, including severe Central Sleep Apnea. This combination of daytime breathing impairment, nighttime oxygen starvation, and the inability to clear lung secretions creates a dangerous cycle of chronic infections, lung collapse (atelectasis), and respiratory failure.
What is Going Wrong & Why
Normal breathing and airway clearance rely on a complex, highly coordinated "bellows" system of muscles. Following an SCI, this system is structurally dismantled:
- The Loss of the "Bellows" (Restrictive Lung Disease): Depending on the level of the lesion, patients lose control of the diaphragm (C3-C5), intercostal rib muscles (T1-T12), and abdominal muscles (T1-L1). This paralysis drastically reduces the chest wall's ability to expand and contract, causing a severe drop in the total volume of air the lungs can hold and move (vital capacity).
- The Paralyzed Cough: A normal, effective cough requires three phases: a deep breath in, the closure of the airway to build pressure, and a violent contraction of the abdominal and intercostal muscles to forcefully expel air and shear mucus off the lung walls. In SCI, the loss of these expiratory muscles makes the expulsive phase incredibly weak or absent, leaving the patient entirely unable to clear their own airway.
- Central Sleep Apnea & "Loop Gain": During sleep, the brain monitors oxygen and carbon dioxide levels to dictate the drive to breathe. After a cervical SCI, the central nervous system frequently develops an abnormally high "loop gain"—meaning the brain's breathing control center becomes highly unstable. This causes the patient to fluctuate wildly between hyperventilation and complete central apneas (where the brain temporarily stops sending the signal to breathe), resulting in repeated, severe drops in blood oxygen (hypoxemia) every night.
The Implications, Long-Term Problems, and Confounding Issues
The inability to breathe deeply or clear the airway leads to gravity pulling normal, daily lung secretions down into the deep peripheral airways where they form intractable mucus plugs. This creates the perfect breeding ground for toxic bacterial colonization, leading to a "vicious circle" of recurrent pneumonia, chronic lung inflammation, and progressive lung tissue destruction.
Confounding Issue 1: "Paradoxical" Breathing
In many lower-cervical or thoracic SCI patients, the diaphragm may still work, but the abdominal and rib muscles do not. Because the ribs and abdomen cannot hold their rigid shape, when the diaphragm pulls down to suck air in, the chest wall actually collapses inward instead of expanding. This "paradoxical breathing" is highly inefficient and exhausts the remaining working muscles, leading to rapid respiratory fatigue.
Confounding Issue 2: The Immobility Factor
In able-bodied individuals, simply walking and moving around naturally aids airway clearance by up to 41%. Exercise increases airflow, thins mucus, and helps mobilize secretions from the deep lungs. SCI patients lose this critical, natural mechanical clearance mechanism due to their paralysis, compounding the danger of their weakened cough.
Confounding Issue 3: The Misdiagnosis of Sleep Apnea
In the general population, sleep apnea is primarily obstructive (frequently driven by obesity blocking the physical airway). While SCI patients can have obstructive apnea, they have staggeringly high rates of central sleep apnea (up to 93% in cervical SCI) due to the neurological damage itself. Healthcare providers who assume the apnea is purely weight-related may miss the profound neuro-ventilatory instability that requires specialized respiratory support.
Current Advice, Treatments & Research Trends
The management of SCI respiratory dysfunction is rapidly evolving from manual therapies to highly advanced bionic and neuro-regenerative technologies.
- Advanced Airway Clearance Therapy (ACT): Because manual chest percussion requires a caregiver and is labor-intensive, treatment relies heavily on technology. Devices like High-Frequency Chest Wall Oscillation (HFCWO) vests deliver automated pneumatic pulses to the chest to shake mucus loose. For actual mucus extraction, Mechanical Insufflation-Exsufflation (MIE) devices (like the CoughAssist) use alternating positive and negative pressure to simulate a forceful cough.
- Biphasic Cuirass Ventilation (BCV): Traditional positive-pressure ventilators (which blow air into the lungs) can damage lung tissue over time and prevent a patient from speaking or eating. BCV is a non-invasive shell (a cuirass) worn over the chest that uses negative pressure to pull the chest open, mimicking normal physiological breathing. This preserves lung volume, improves cardiac output, and allows the patient to eat, speak, and retain their independence.
- Abdominal Functional Electrical Stimulation (FES): To give patients their cough back, clinicians are using FES applied directly to the paralyzed abdominal muscles. When the patient needs to cough, electrical pads force the abdominal muscles to violently contract, providing the vital "expulsive force" needed to clear the airway and preventing the need for frequent tracheal suctioning.
- Therapeutic Acute Intermittent Hypoxia (tAIH): One of the most groundbreaking regenerative treatments currently in clinical trials is tAIH. Patients breathe brief, 1-minute bursts of low-oxygen air (around 9-10% oxygen) alternated with normal air. This mild, controlled "oxygen stress" tricks the brain into releasing serotonin and Brain-Derived Neurotrophic Factor (BDNF) directly into the spinal cord. This biochemical cascade strengthens the remaining intact neural pathways to the diaphragm and intercostals, actively restoring the patient's natural ability to take deeper, stronger breaths without relying solely on mechanical support.
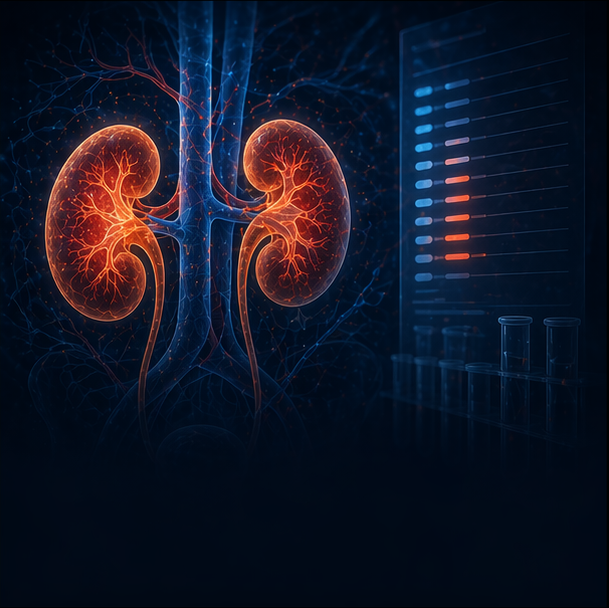
6. The Kidney Test Trap & Silent Renal Toxicity
Brief Summary of the Problem
Following a spinal cord injury (SCI), individuals experience a massive and permanent loss of muscle mass. Because standard medical tests rely on muscle waste products to measure how well the kidneys are filtering blood, this extreme muscle loss essentially "breaks" the standard kidney test, making failing kidneys look perfectly healthy on paper. This "Kidney Test Trap" is highly dangerous because doctors, believing the kidneys are fine, will prescribe standard doses of heavy, renally-cleared medications like Baclofen and Gabapentin. Unable to be filtered out, these drugs silently accumulate in the blood to highly toxic levels, poisoning the brain and causing severe, life-threatening neurological emergencies that are frequently misdiagnosed.
What is Going Wrong & Why
To understand the trap, you must understand how doctors measure kidney function, known as the Glomerular Filtration Rate (eGFR).
In a standard clinical setting, eGFR is calculated using a blood test for Creatinine. Creatinine is a chemical waste product generated by normal muscle metabolism. In an able-bodied person, the amount of muscle is relatively stable, so if creatinine levels in the blood rise, it means the kidneys are failing to filter it out.
However, after a motor-complete SCI, the paralyzed sublesional muscles undergo an obligatory and severe atrophy (sarcopenia). Because the patient has lost a massive percentage of their metabolically active muscle, their body produces very little creatinine.
The Layman's Translation: Imagine trying to figure out how busy a restaurant is by looking at how many dirty plates are piled up in the sink. If the restaurant has no customers (no muscle), the sink will be empty. The manager (the doctor) looks at the empty sink and assumes the dishwasher (the kidney) is working perfectly and doing a great job. In reality, the dishwasher might be completely broken; there are just no plates to pile up and show it.
Because of this physiological illusion, standard creatinine-based eGFR equations consistently and dangerously overestimate kidney function in SCI patients by up to 50%.
The Implications, Long-Term Problems, and Confounding Issues### Masked Chronic Kidney Disease (CKD)
The most immediate implication is that Chronic Kidney Disease (CKD) goes completely undiagnosed. In studies adjusting for the SCI muscle-loss factor, researchers found that over 1 in 3 SCI patients actually have hidden CKD—a rate more than three times higher than what traditional creatinine tests report.
The Confounding Issue: The Polypharmacy Toxidrome
The true danger of the eGFR illusion lies in medication dosing. People with chronic SCI frequently rely on medications like Baclofen (for severe spasticity) and Gabapentin (for neuropathic pain). Both of these medications are not processed by the liver; they are 70% to 80% excreted entirely unchanged by the kidneys.
Because the patient's creatinine test falsely claims their kidneys are healthy, doctors prescribe standard or high doses of these drugs. Because the hidden kidney failure prevents the drugs from being cleared, they pool in the bloodstream and cross the blood-brain barrier.
Silent Renal Toxicity & Encephalopathy
This accumulation leads to "Baclofen-induced neurotoxicity" or "metabolic encephalopathy". The patient is essentially poisoned by their own medication. This presents with severe, atypical symptoms:
- Profound, unarousable sleepiness, lethargy, and cognitive "brain fog".
- Myoclonus (sudden jerky muscle movements) and loss of motor coordination (leading to dangerous wheelchair falls).
- Severe respiratory depression.
- In extreme cases, the toxicity can induce a coma that is so deep it mimics clinical brain death.
Because doctors are unaware of the underlying kidney failure, these toxic episodes are frequently and dangerously misdiagnosed as strokes, sudden dementia, or severe psychiatric crises. Interestingly, an unusual, "silent" warning sign of impending Baclofen toxicity is the sudden onset of intractable hiccups alongside unusual drowsiness or a "blank stare".
Current Advice, Treatments & Research Trends
To prevent toxic medication build-up, clinical practice for the SCI population is undergoing a major diagnostic shift.
- The Diagnostic Fix (Demand Cystatin C): Healthcare providers must abandon serum creatinine as the sole marker for kidney function in SCI. Patients must advocate for a Cystatin C blood test. Cystatin C is a low-molecular-weight protein produced at a constant rate by all nucleated cells in the body, meaning it is completely unaffected by muscle mass, age, or diet. Research conclusively proves that using the CKD-EPI Cystatin C equation provides a highly accurate, unbiased measurement of true kidney function in paralyzed individuals.
- Renal-Adjusted Dosing ("Start Low, Go Slow"): Once true kidney function is established via Cystatin C, doctors must rigorously adjust medication dosages. For patients with even mild-to-moderate hidden renal impairment (eGFR between 30 and 80 mL/min), Baclofen and Gabapentin doses must be proactively reduced and strictly monitored to avoid encephalopathy.
- Emergency Toxicity Management: If a patient presents with sudden, unexplained encephalopathy, lethargy, or intractable hiccups, providers must immediately suspect baclofen/gabapentin toxicity. Because Baclofen has a low molecular weight and low protein-binding capacity, it is highly dialyzable. In severe toxic emergencies, emergent hemodialysis is the most effective treatment to rapidly clear the drug from the blood and restore brain function.
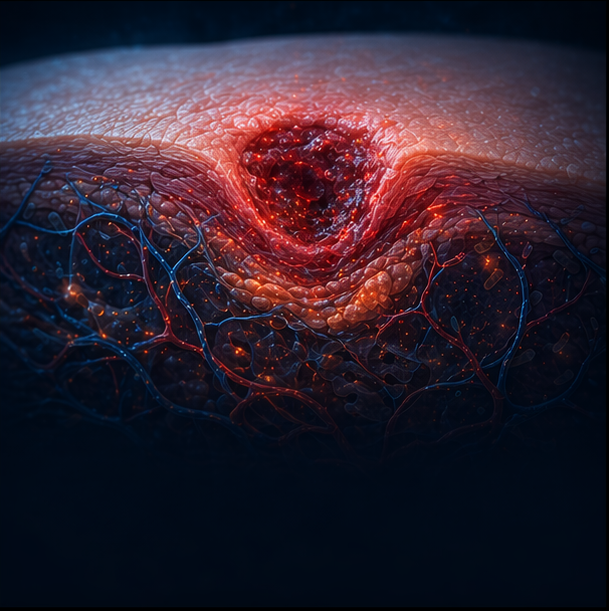
10. Refractory Pressure Injuries & Microvascular Dysfunction
Brief Summary of the Problem
Pressure injuries (PIs), or bedsores, are a relentless and severe complication of chronic spinal cord injury (SCI). While often thought of simply as the result of "sitting in one spot too long," refractory (non-healing) pressure injuries in the SCI population are actually driven by a profound systemic failure. The combination of paralyzed micro-blood vessels, severe muscle atrophy, and a system-wide inflammatory state creates a highly toxic, oxygen-starved wound environment. This prevents the body's normal cellular repair mechanisms from functioning, turning a minor skin breakdown into a chronic, deep-tissue wound that can lead to bone infection, amputation, and life-threatening sepsis.
What is Going Wrong & Why
The development of non-healing pressure injuries in SCI is driven by a breakdown in three critical physiological systems:
- Microvascular Collapse & Ischemia: The loss of autonomic nervous system control severely impairs vascular tone and microcirculation below the level of the injury. Normal skin relies on a dynamic, responsive blood supply to deliver oxygen and regulate temperature. In SCI, the blood vessels cannot adapt to sustained pressure, leading to rapid ischemia (oxygen starvation) and localized tissue death (necrosis).
- The Loss of the "Muscle Cushion": Severe muscle atrophy and the replacement of lean mass with fatty tissue radically alter the body's composition. The robust muscle tissue that usually acts as a protective shock-absorber over bony prominences (like the sitting bones) wastes away, leaving fragile skin compressed directly between bone and wheelchair surfaces.
- The Macrophage Trap (Blocked Healing): In a healthy body, immune cells called macrophages arrive at a wound in an aggressive, pro-inflammatory state (M1) to clear out dead tissue, and then transition into a reparative state (M2) to actively rebuild the tissue. In chronic SCI, the toxic, highly inflammatory systemic environment (driven by adipokines like IL-1, IL-6, and TNF- $\alpha$) traps the macrophages in the destructive pro-inflammatory phase. This halts the healing process entirely, delaying the critical M2 transition needed to close the wound.
The Implications, Long-Term Problems, and Confounding Issues
Deep, refractory pressure injuries drastically reduce a patient's quality of life, frequently requiring months of complete bed rest, surgical flap procedures, and heavy antibiotic use that further destroys the gut microbiome.
Confounding Issue 1: The "Silent" AD Trigger
In individuals with injuries at or above T6, a major confounding issue is that a pressure sore acts as a massive, constant noxious stimulus to the nervous system. Even though the patient cannot feel the pain of the wound, the body perceives the tissue damage. Skin issues, including pressure injuries at any stage, are the third most common trigger for Autonomic Dysreflexia (AD). A hidden pressure sore can drive a patient into a chronic state of "silent" hypertensive AD spikes, risking a stroke without the patient or provider realizing a wound is causing the cardiovascular emergency.
Confounding Issue 2: Standard Wound Care is Insufficient
Standard wound care for able-bodied patients assumes the body has the fundamental vascular and cellular tools to heal once pressure is relieved. Healthcare providers must understand that in SCI, relieving the pressure is only half the battle. Because the local micro-environment lacks adequate blood flow and the immune cells are stuck in an inflammatory loop, simply turning the patient and applying standard dressings will often fail to resolve the wound.
Current Advice, Treatments & Research Trends
To overcome the physiological barriers to wound healing, clinical management is increasingly incorporating bio-engineering, advanced stimulation, and targeted energy therapies.
- Bionic Blood Flow (Electrical Stimulation): Researchers are utilizing Functional Electrical Stimulation (FES) both as prevention and treatment. Applying FES to the gluteal muscles while the patient is sitting forces the paralyzed muscles to contract, which actively lowers peak seating pressure and mechanically pumps blood under the sitting bones to prevent ulcers. For active wounds, applying gentle electrical currents around a chronic ulcer has been shown in randomized trials to significantly speed healing and shrink the wound by boosting local blood flow and drawing healing cells into the cavity.
- Photobiomodulation (Red/NIR Light Therapy): The application of specific therapeutic wavelengths of red and near-infrared (NIR) light (between 600 nm and 900 nm) is emerging as a powerful, non-invasive tool. This light penetrates deep into the tissue to stimulate cellular energy production, actively reduce local inflammation, and promote tissue repair. Combining this with far-infrared (FIR) heat lamps provides gentle thermal therapy that dilates local blood vessels, further increasing the oxygen supply to the starved tissue.
- Low-Intensity Ultrasound Therapy: High-frequency, low-intensity ultrasound is being used to actively reverse the vascular dysfunction in the wound bed. Ultrasound mechanical waves stimulate the expression of Vascular Endothelial Growth Factor (VEGF), which triggers angiogenesis—the formation of brand new, healthy blood vessels—directly within the damaged tissue, re-establishing the critical nutrient supply required for wound closure.
Chronic Inflammation After SCI: What Research Says We Can Do Every Day
Brief Summary of the Problem
Living with a chronic spinal cord injury (SCI) often means living in a persistent, low-grade state of immune activation. This is sometimes described as parainflammation or inflammaging. It is not the short, useful burst of inflammation that helps heal a cut or fight off a virus. Instead, it is more like a quiet background fire that keeps smoldering year after year. In SCI, that fire is often fed by changes in body composition, slowed bowel function, disrupted gut bacteria, recurrent infections, skin stress, reduced muscle activity, and other secondary complications.
Over time, this chronic inflammation can act as a master amplifier for many of the major long-term problems seen after SCI. It is linked to worse cardiometabolic health, faster biological aging, higher vascular risk, hormone disruption, and greater neuropathic pain. The encouraging part is that research increasingly shows this inflammatory load is not completely fixed. Everyday choices, especially around diet, gut health, and activity, can help cool it down.
What is Going Wrong & Why
The chronic inflammatory state seen after SCI is usually not caused by one single problem. It is driven by a self-reinforcing loop involving fat tissue, the gut, reduced movement, and repeated secondary stressors.
- The "Fat Factory" (Visceral Fat & Adipokines): After SCI, loss of muscle mass and a lower metabolic rate make it much easier to gain visceral fat around the organs. This fat is not just stored energy. It behaves like an active chemical organ and releases inflammatory messengers called adipokines, including molecules such as Interleukin-6 and TNF-α. In other words, excess visceral fat can continuously drip inflammatory signals into the bloodstream.
- The "Leaky Gut" Problem (Dysbiosis & Endotoxemia): SCI slows bowel motility and changes the gut environment. Food and waste may sit in the bowel longer, beneficial bacteria can decline, and more harmful bacteria can overgrow. This imbalance is known as dysbiosis. Over time, the lining of the gut can become more permeable, allowing bacterial components such as lipopolysaccharides (LPS) to pass into the bloodstream. This is sometimes called endotoxemia, and it can trigger wide-reaching immune activation.
- The Loss of Anti-Inflammatory Muscle Signals: Active muscle does more than create movement. It also releases anti-inflammatory signaling molecules known as myokines. After SCI, reduced muscle activation means the body loses an important built-in brake on inflammation.
- The "Constant Alarm" of Secondary Complications: With SCI, the immune system may be repeatedly triggered by silent or recurring problems such as urinary tract infections, bladder irritation, bowel dysfunction, microscopic skin breakdown, respiratory issues, and episodes of Autonomic Dysreflexia (AD). Even when these problems are not dramatic, they can keep the immune system stuck in a constant state of alert.
The Implications, Long-Term Problems, and Confounding Issues
When the body is exposed to chronic low-grade inflammation for years, the damage is not always obvious day to day, but it can be significant over time.
This inflammatory state is strongly linked to:
- Worse neuropathic pain: Inflammatory chemicals can make nerve pathways more irritable and hypersensitive.
- Cardiovascular and metabolic disease: Chronic inflammation damages blood vessels and increases risk for insulin resistance, atherosclerosis, and broader cardiometabolic decline.
- Hormonal disruption: In men especially, inflammatory diets and chronic inflammatory burden are linked to lower testosterone, particularly when combined with increased body fat.
- Accelerated biological aging: The inflammatory load in chronic SCI appears to push the body toward an earlier and more aggressive aging profile.
Confounding Issue 1: The Blood Test Trap
In the general population, mildly raised inflammatory markers may be dismissed as a temporary illness or a minor infection. In SCI, slightly elevated markers such as hs-CRP or Interleukin-6 may actually reflect the person’s chronic baseline inflammatory state rather than a one-off event. Because the person may not look visibly ill, these warning signs can be underappreciated even though they may be signaling increased long-term cardiometabolic risk.
Confounding Issue 2: The "Healthy Diet" That Still Falls Short
A person with SCI may genuinely eat well but still struggle with inflammation because the gut is not functioning normally. If the gut lining is inflamed and absorption is impaired, important nutrients may not be absorbed properly. This means someone can appear to be doing the right things on paper but still have ongoing nutrient shortfalls that weaken the body’s anti-inflammatory defenses.
Confounding Issue 3: Standard Advice Does Not Always Translate Directly to SCI
General anti-inflammatory advice often tells people to simply eat more fibre, move more, and lose weight. Those principles still matter in SCI, but they usually need adaptation. For example, suddenly increasing fibre without enough water can worsen bowel problems in SCI rather than help them. Likewise, physical activity may need to come from upper-body exercise, FES cycling, or other assisted movement rather than standard able-bodied exercise advice.
Current Advice, Treatments & Everyday Strategies
Research increasingly supports a practical, everyday anti-inflammatory approach for SCI that focuses on diet quality, gut support, and whatever safe movement is possible.
- Use an Anti-Inflammatory Diet as a Daily Base: A randomized controlled trial in people with chronic SCI found that a strict 12-week anti-inflammatory diet reduced inflammatory biomarkers and also improved neuropathic pain severity. Current guidance increasingly points toward a Mediterranean-style or Mediterranean Plus approach, with some evidence also supporting more plant-forward patterns. The common theme is simple: build the diet around minimally processed foods that calm inflammation rather than fuel it.
- Prioritize Omega-3 Fats: Omega-3-rich foods such as salmon, mackerel, sardines, walnuts, and other oily fish or nuts are among the most important anti-inflammatory foods discussed in SCI-related research. They provide the building blocks for specialized pro-resolving mediators (SPMs), which help actively switch off inflammation once it has done its job. Studies in SCI have also reported improvements in inflammatory markers with Omega-3 supplementation, sometimes alongside vitamins A and D. Daily fish oil in the region of 3,000 mg has been associated with improvements in markers such as CRP and the neutrophil-to-lymphocyte ratio (NLR).
- Feed the Gut Bacteria That Help You: High-fibre foods, resistant starches, and prebiotic foods help nourish beneficial gut bacteria. When those bacteria ferment fibre, they produce short-chain fatty acids (SCFAs) such as butyrate, acetate, and propionate. These are not just gut by-products. They are important anti-inflammatory signaling molecules that help strengthen the intestinal barrier, reduce gut leakiness, and suppress inflammatory pathways including TNF-α and IL-6.
- Think "Fibre Plus Water," Not Fibre Alone: In SCI, this is a major practical difference from general population advice. Increasing fibre can be helpful, but only when paired with adequate fluid intake and bowel tolerance. Without enough water, extra fibre may worsen constipation or contribute to bowel obstruction risk rather than improve gut health.
- Use Polyphenols, Spices, and Antioxidant-Rich Foods Regularly: Colorful fruits and vegetables, extra virgin olive oil, berries, green tea, turmeric, and ginger all provide phytonutrients and antioxidants that help counter oxidative stress and support healthier inflammatory profiles.
- Reduce the Foods That Keep the Fire Burning: Strong evidence links ultra-processed foods, refined carbohydrates, added sugars, and trans fats with higher systemic inflammation. These foods can also encourage harmful shifts in the gut microbiome. In SCI, diets high in fat and sugar may be particularly unhelpful because they may worsen metabolic dysfunction and may even interfere with a more repair-friendly biological environment.
- Move What Can Be Moved: Movement remains anti-inflammatory medicine even in paralysis. Where appropriate, upper-body exercise, Functional Electrical Stimulation (FES) cycling, or other electrically assisted movement can stimulate muscle activity and release anti-inflammatory myokines. This matters not only for fitness, but for inflammatory balance.
- Take Silent Inflammation Seriously: Everyday management of bowel care, bladder care, skin protection, pressure relief, and infection prevention is also anti-inflammatory care. In SCI, the body does not need a dramatic crisis to stay inflamed. Small, repeated stressors can be enough to keep the immune system activated.
What This Means in Real Life
For many people with SCI, the most realistic anti-inflammatory strategy is not a perfect diet or a miracle supplement. It is a steady pattern of daily choices that reduce inflammatory pressure from multiple angles at once.
That usually means:
- building meals around whole, minimally processed foods
- getting regular Omega-3 intake
- supporting the gut microbiome with fibre, prebiotics, and hydration that match bowel tolerance
- reducing high-sugar, highly processed foods
- treating bowel, bladder, skin, and infection prevention as part of inflammation control
- using whatever safe movement or muscle activation is possible
The key idea is that in SCI, inflammation is often not just something that happens during illness. It can become part of the background biology of daily life. The research suggests that this background can, at least to a meaningful degree, be influenced.
Research Direction & Bigger Picture
One of the most interesting shifts in SCI research is that inflammation is increasingly being viewed not just as a side issue, but as part of the core long-term biology of living with SCI. Researchers are paying much closer attention to the links between gut health, body fat, immune signaling, pain, metabolism, and aging.
This does not mean diet alone can reverse chronic SCI. But it does mean that diet and lifestyle may help shape the biological environment in which everything else happens. A lower-inflammatory body may be better positioned for better long-term health, better pain control, and possibly a more supportive background for rehabilitation and future restorative therapies.
SCI Abdominal Distension ("SCI Belly" / "Quad Belly"): What It Is, Why It Happens, and What Can Help
Brief Summary of the Problem
Abdominal distension after spinal cord injury, often called "SCI belly" or "quad belly" in the community, is a very real and very common problem, especially after cervical and higher thoracic injuries. It is not just ordinary weight gain, and it is not simply a cosmetic issue. In most cases it is the visible result of several problems stacking on top of each other: the abdominal wall becomes weak or paralysed, the bowel slows down and holds onto stool and gas, seated posture collapses forward, and body composition changes over time.
That is why a person can look relatively slim in their face, arms, and legs, yet still develop a large, firm, or protruding abdomen. This mismatch can be confusing and upsetting, especially because standard measures like BMI often do a poor job of reflecting what is really happening in the SCI body.
The important point is this: SCI abdominal distension is usually a combined trunk-control, bowel, breathing, and body-composition problem. The belly is not just “bigger”. The whole support system around the abdomen has changed.
What is Going Wrong & Why
Abdominal distension after SCI is best understood as a multi-part mechanical and neurological problem rather than one single diagnosis.
- The abdominal wall loses its normal "corset" function: In a non-injured body, the rectus abdominis, obliques, and transversus abdominis act like a living support belt. They help hold the abdominal contents in, support posture, help with coughing, and assist with bearing down. After SCI, especially with injuries above the lower thoracic levels, those muscles can become profoundly weak or paralysed. Over time they often thin and atrophy. In plain English, the front wall of the abdomen stops acting like a firm support and becomes much more like a slack container.
- The bowel becomes slower and less efficient: Neurogenic bowel is one of the biggest drivers of abdominal distension. Food and waste move more slowly through the gut after SCI, and the person may not empty fully or regularly. This allows faecal loading, fermentation, and gas build-up. The result is the familiar mix of fullness, pressure, bloating, visible swelling, and days when the abdomen seems to change shape or size.
- Gas becomes trapped more easily: Slow transit gives gut bacteria more time to ferment food, especially certain carbohydrates. At the same time, weak abdominal muscles make it harder to generate the pressure needed to move gas along or expel it. So the abdomen is not only fuller, it is also less able to “clear itself”.
- Posture makes the problem look even larger: A lot of people describe the belly as looking as though it is tipping or hanging forward. The research literature describes this a few different ways depending on the exact seating pattern, but the practical point is the same: when trunk muscles are weak, the torso slumps, the rib cage and pelvis stop stacking well, and the abdominal mass projects outward. In other words, posture can make the same amount of internal pressure look much worse from the outside.
- Body composition changes complicate the picture: After SCI, muscle mass often drops while body fat, especially around the centre, can increase even if body weight does not rise dramatically. This is one reason BMI can look “fine” while the abdomen still becomes much more prominent.
- The abdominal wall itself may structurally change over time: In long-standing paralysis, muscle tissue can gradually be replaced by more fatty and fibrous tissue. That matters because fibrous, stretched tissue does not behave like healthy contractile muscle. This is one reason long-established abdominal distension can become difficult to reverse fully with ordinary exercise alone.
A useful way to picture the whole problem is this: the belly is being pushed from the inside, held less effectively from the outside, and made more visible by slumped trunk mechanics.
The Implications, Long-Term Problems, and Confounding Issues
Abdominal distension after SCI is often dismissed as a body-shape issue, but in reality it can affect several important parts of daily life and health.
- Breathing can become less efficient: The diaphragm works best when the abdomen gives it something firm to push against. When the abdominal wall is slack and the abdomen is already distended, the diaphragm loses some of that support. This can reduce breathing efficiency, weaken cough, and make it harder to clear secretions. In people who already have limited respiratory reserve, this matters.
- Bowel symptoms can spiral: Distension and bowel dysfunction often feed each other. Constipation leads to more loading and bloating, bloating makes the belly feel tighter and more uncomfortable, and that can make eating, positioning, and bowel care harder.
- Sitting balance and comfort can worsen: The visible belly is often one sign of a broader trunk-instability problem. A person may feel more slumped, less balanced, less supported, and less efficient during transfers or reaching. In a wheelchair, poor trunk alignment can also affect straps, supports, and overall comfort.
- Skin and moisture problems can increase: Poor posture, bowel issues, moisture, incontinence, and compression from clothing or equipment can all raise skin risk. The evidence is stronger for this combined effect than for belly size alone, but clinically it is still important.
- Autonomic dysreflexia can sometimes be part of the picture: In people at risk of AD, bowel loading, constipation, gas, or severe bowel irritation can act as triggers. So in some people the distension is not only uncomfortable, it may sit inside a more serious autonomic problem.
- Body image distress can be significant: Many people with SCI describe the strange experience of feeling “thin everywhere else” yet having a belly that looks out of proportion to the rest of the body. This can create shame, frustration, social withdrawal, and a sense that the body no longer looks or feels like “you”.
Confounding Issue 1: The BMI Trap
One of the biggest sources of confusion is that BMI is often misleading in SCI. A person may have a normal or even low BMI while still carrying greater central fat and having obvious abdominal protrusion. So someone can feel as though they “look overweight” while standard weight measures say otherwise.
Confounding Issue 2: It Is Not Just Fat
Many people understandably assume the belly is simply fat gain. Fat can be part of it, but the overall problem usually includes muscle denervation, bowel loading, gas trapping, posture, and altered breathing mechanics. That is why dieting alone often does not solve it.
Confounding Issue 3: More Fibre Is Not Always Better
General health advice often says “eat more fibre” for bloating or constipation. In SCI, that can backfire if bowel motility is poor or fluid intake is not adequate. Extra fibre without enough water, timing, and motility can increase bulk and worsen the feeling of blockage or fullness. The better approach is individualised fibre, not automatic high fibre for everyone.
Confounding Issue 4: Different People Mean Different Things by "Posture"
Some people describe the problem as a forward-tipped pelvis. Others are clearly dealing with a slumped, rounded, C-shaped seated posture. Both descriptions can be true in practice, because the main issue is not one single textbook posture. It is that the trunk is no longer being actively held in an efficient way.
Current Advice, Treatments & Everyday Strategies
At the moment, there is no single standard treatment that permanently fixes SCI abdominal distension. Current management is usually about improving the different contributors rather than chasing one magic answer.
- Start with bowel management, because this is often the biggest day-to-day driver: A consistent bowel programme remains central. That may include timing bowel care around the gastrocolic reflex after meals, making sure rectal emptying is effective, adjusting stool-softening or stimulant medications when needed, and reviewing whether the current routine is actually preventing loading or simply managing it incompletely.
- Treat constipation first when bloating is a major issue: This sounds basic, but it is one of the most important clinical messages in the literature. If stool is sitting there, the abdomen is already under internal pressure. Until that is addressed, other strategies may only partly help.
- Review food triggers realistically: Some people do better by reducing foods that are very gas-producing or poorly tolerated. Depending on the person, that might include certain dairy foods, highly fermentable carbohydrates, fizzy drinks, or individual trigger foods identified by experience. For some people, a more Mediterranean-style eating pattern or even a carefully trialled lower-FODMAP approach can reduce bloating.
- Think in terms of fibre plus fluid plus tolerance: Fibre can help some people, but only when it matches the person’s bowel pattern, fluid intake, and tolerance. The goal is not simply “more fibre”. The goal is better stool consistency and easier movement through the bowel.
- Abdominal or colonic massage can help some people: This is one of the more practical strategies mentioned in both guidance and lived experience. It does not repair the abdominal wall, but it may help move trapped gas or stool along.
- Positioning matters more than many people realise: Frequent pressure-relief movements, side leans, changes in seating angle, prone lying when feasible, and improving how the rib cage and pelvis are supported can all make a visible difference. Sometimes the belly looks less “dramatic” not because the bowel changed overnight, but because the trunk is being held better.
- Abdominal binders can help, but they are not perfect: A binder can act like an external support where the abdominal wall no longer can. Some people notice better posture, a flatter appearance, improved cough, or easier breathing when upright. But binders also come with trade-offs: they can feel hot, restrictive, awkward for bowel care, or irritating to the skin. They are a tool, not a cure.
- Functional Electrical Stimulation (FES) is promising in some settings: Abdominal or trunk-focused stimulation can improve cough, expiratory function, sitting balance, and in some cases muscle thickness or trunk control. That makes it one of the more interesting rehabilitation options. However, it is still not a simple, standardised everyday fix for abdominal contour, and bowel-focused abdominal FES is still more research-track than routine clinical default.
- Seating and wheelchair set-up deserve serious attention: Because this is partly a trunk-control problem, seating matters. Back support, seat angle, pelvic position, laterals, belts, and how the person tends to slump through the day can all influence how prominent the abdomen appears and how supported the person feels.
- Gas-management strategies may help some people: Simethicone or similar anti-flatulents are sometimes used, though results vary. Keeping a food-and-symptom diary can be surprisingly useful, because many people find their belly has predictable triggers even within the bigger SCI pattern.
- Psychological impact should not be brushed off: Distress about abdominal appearance is not vanity. For many people it is tied to identity, confidence, intimacy, clothing, and how visible their disability feels. Supportive discussion and practical problem-solving matter.
When It Needs Prompt Medical Attention
Although SCI abdominal distension is often chronic and familiar, there are times when it should be treated as a more urgent medical issue.
Medical review is important if abdominal distension is becoming rapidly worse, especially if it comes with:
- worsening nausea or vomiting
- severe constipation or inability to pass stool or gas
- new or severe abdominal pain
- reduced appetite together with marked swelling
- breathing becoming harder than usual
- signs of autonomic dysreflexia
- fever or concern about infection
In SCI, bowel problems can sometimes escalate into ileus, severe faecal loading, respiratory compromise, or AD-related emergencies. A “usual big belly” that suddenly becomes much more severe is worth taking seriously.
What This Means in Real Life
For most people, the most accurate message is not “this is just fat” and not “there is nothing you can do”. The truth sits in the middle.
For many people with SCI, abdominal distension improves most when they treat it as a combined systems problem:
- better bowel emptying
- less stool and gas retention
- smarter food choices based on personal triggers
- better seating and trunk positioning
- selective use of abdominal support
- muscle activation where possible
- realistic expectations about what is structural versus what is changeable
That can be frustrating, because it means the answer is often layered rather than simple. But it also means there are usually multiple points where things can improve, even if the abdomen never returns to a pre-injury look.
Research Direction & Bigger Picture
One of the most encouraging developments is that researchers are increasingly treating this as a real, multi-system SCI problem rather than a cosmetic complaint.
The most realistic near-term hope appears to be neuromodulation, especially:
- transcutaneous spinal stimulation, which may improve posture and trunk control non-invasively
- epidural stimulation, which may provide a more powerful “internal bracing” effect by re-engaging trunk-related spinal networks
- targeted abdominal or trunk stimulation, which may improve cough, posture, and possibly aspects of bowel management
This is promising because it moves beyond squeezing the abdomen from the outside and toward trying to restore some of the support from the inside.
There is also growing interest in:
- better bowel-directed stimulation strategies
- more tailored microbiome and motility approaches for bloating
- smarter prokinetic medications
- muscle-preserving or regenerative approaches
That said, it is important to stay realistic. Right now, the evidence is strongest for conservative management plus selective stimulation-based rehabilitation, while more ambitious muscle-restoring and regenerative approaches remain much earlier-stage.
A major research gap is that patients clearly recognise this problem, but the formal literature still does not study it very often under the same name patients use. In other words, the condition is real, but the research language around it is still catching up with lived experience.
The SCI "Salt Paradox": Eat or Don’t Eat. Bones vs. Blood Pressure
(Disclaimer: The following information is based on current medical research and literature for educational purposes. It is not medical advice. Individuals with SCI should always consult their physician and utilize 24-hour urine testing and blood pressure monitoring before altering their dietary sodium or fluid intake).
On documenting the ten secondary complications of chronic SCI, I discovered that there were conflicting advice on salt intake. In protecting bones & reducing calcium stones (lessen those catheter blockages) the advice very reduced salt diet. However if like me you get low blood pressure (orthostatic hypotension – OH), especially after eating leading to dizziness & feeling ‘crap’ until it wears off, the advice is to ingest salt. So I looked to the experts & the information is as follows (& still on the fence, but does offer alternatives).
The Conflict Explained In the general, able-bodied population, the advice is simple: eat less salt. But an SCI fundamentally alters both cardiovascular and renal (kidney) physiology, creating a dangerous tug-of-war:
- Why your Kidneys & Bones hate salt: High dietary sodium actively forces the kidneys to excrete more calcium into the urine (a process where sodium "drags" calcium out with it). For someone with SCI who is already suffering from rapid bone demineralization, high salt accelerates bone loss and severely increases the risk of calcium-based kidney stones. Because of this, general guidelines for stone formers recommend restricting sodium to less than 1,500 mg to 2,400 mg daily.
- Why your Blood Pressure needs salt: Individuals with high-level SCI (T6 and above) lose sympathetic nervous system control over their blood vessels, meaning the vessels cannot "squeeze" to fight gravity. This causes massive blood pooling in the abdomen and legs, leading to Orthostatic Hypotension (OH)—dangerous drops in blood pressure when sitting up. To fight this, patients are often advised to consume extra salt and water to artificially expand their total blood volume and keep their blood pressure stable.
So, how do you decide how much salt to consume? The medical literature explicitly notes that there are currently no official guidelines that perfectly unify water and salt intake for SCI patients managing both conditions simultaneously. However, clinical research reveals four strategies to help patients navigate this paradox:
1. Determine Your True Risk Profile (Level of Injury Matters)
The need for salt is highly dependent on the neurological level of the injury.
- Lower-Level Injuries (Below T6): These individuals generally have intact sympathetic vascular control and do not suffer from severe neurogenic orthostatic hypotension. For this group, there is no cardiovascular benefit to consuming extra salt. They should strictly follow the low-salt diet (≤ 2,400 mg/day) to protect their bones, prevent kidney stones, and reduce the risk of cardiometabolic disease.
- High-Level Injuries (T6 and Above): This group is uniquely at risk for both severe OH and Autonomic Dysreflexia (AD). For them, preventing a hypotensive "crash" that starves the brain of oxygen is a daily emergency, which often justifies a higher salt intake.
2. Timing Over Total Volume (The "Morning" Strategy)
If an individual with a high-level SCI needs salt to maintain blood pressure, when they consume it is more important than simply eating a high-salt diet all day.
- Research indicates that orthostatic stress and blood pressure crashes are most severe in the morning (after the body has been horizontal all night and is suddenly subjected to the gravity of a wheelchair transfer).
- Therefore, targeting a controlled salt/fluid intake specifically in the morning or mid-morning can provide the necessary blood volume expansion to survive daytime rehabilitation and upright sitting, without requiring the patient to consume massive amounts of sodium during dinner or at night. This targeted approach prevents the kidneys from being bombarded with a 24-hour continuous stream of high sodium.
3. The Hydration Bridge (Diluting the Danger)
Salt only expands blood volume if it holds onto water. Simultaneously, water is the absolute best defense against kidney stones.
- If a patient must increase their salt intake to manage OH, they must aggressively increase their water intake alongside it. Clinical studies show that maintaining a high fluid volume expands the extracellular fluid to stabilize blood pressure.
- Simultaneously, this massive hydration ensures the patient produces at least 2.5 liters of urine per day. The high volume of water dilutes the calcium that the salt is dragging into the bladder, significantly lowering the "supersaturation" of the urine and preventing the calcium from crystallizing into stones.
4. Leaning on Non-Dietary OH Interventions
If a patient has a severe history of kidney stones or severe osteoporosis, manipulating salt may simply be too dangerous. In these cases, the literature recommends aggressively managing the Orthostatic Hypotension mechanically rather than nutritionally.
- Mechanical Compression: Using medical-grade abdominal binders and tight compression stockings physically squeezes the blood out of the legs and abdomen, doing the job of the paralyzed blood vessels without the need for dietary salt.
- Bionic Muscle Pumps: Utilizing Functional Electrical Stimulation (FES) on the leg muscles while sitting forces the muscles to contract, artificially pumping blood back to the heart to stabilize blood pressure.
Summary: If you have a T6 or higher injury and pass out when you sit up, morning salt and water loading is a valid, clinically recognized tool to keep your brain oxygenated. However, you cannot do this blindly. You must drink massive amounts of water to keep your kidneys flushed, and you should ask your doctor for a 24-hour urine collection test. If that test shows your body is dumping dangerous levels of calcium, you may need to reduce your salt and rely on abdominal binders and compression stockings to manage your blood pressure instead.